For decades, the medical community and the public alike viewed obesity through a narrow lens: a simple imbalance of “calories in versus calories out.” But as we delve deeper into the Metabolic Nexus, it has become clear that obesity is not a lifestyle choice—it is a complex, chronic, and relapsing metabolic disease that sits at the center of a much larger web of complications.
Shifting our clinical perspective is essential. To tackle the crises of Type 2 Diabetes, Heart Disease, and Kidney failure, we must focus on the key factor: Obesity.
1. The Intersection of Science and Physiology
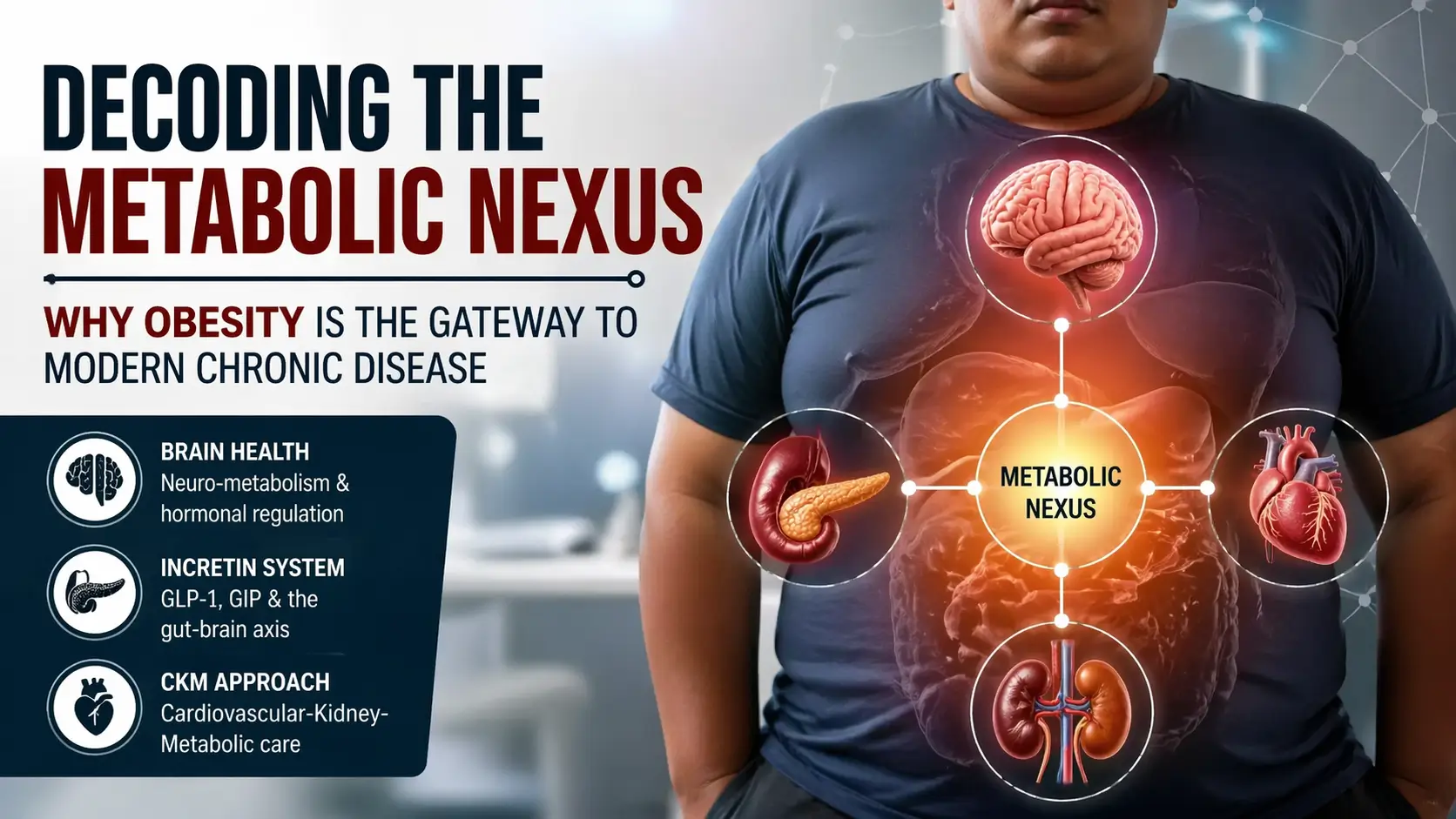
The “Metabolic Nexus” refers to the interconnected nature of our body’s vital systems. Obesity doesn’t exist in a vacuum; it triggers a cascade of inflammatory and hormonal responses that impact:
- The Brain (Neuro-metabolism): The hypothalamus acts as the body’s thermostat. In obesity, this thermostat is often “reset” to a higher weight, making it physiologically difficult for patients to maintain weight loss through willpower alone.
- The Incretin System: The gut-brain axis, governed by hormones like GLP-1 and GIP, is often impaired. This is why the new generation of incretin-based therapies is proving so transformative—they aren’t just “weight loss drugs”; they are metabolic regulators.
2. The CKM Framework: A New Standard of Care
One of the core pillars is the transition toward the Cardiovascular-Kidney-Metabolic (CKM) approach.
Traditionally, a patient might see a cardiologist for their heart, a nephrologist for their kidneys, and a diabetologist for their sugar. However, these conditions are often branches of the same tree. By focusing on the “Metabolic Nexus,” we can:
- Screen Early: Identify metabolic dysfunction before it manifests as end-organ damage.
- Treat Holistically: Use therapies that offer cardiorenal protection while simultaneously managing weight and glucose.
3. Implementing the “Obesity Clinic” Protocol
Theory is only as good as its application. In the presentation, I outlined a practical workflow for a modern metabolic unit. This involves:
- Empowering Healthcare Assistants (HCAs): Training staff to conduct standardized screenings, including BMI, waist circumference, and sarcopenia (muscle loss) assessments.
- Precision Medicine: Moving away from “one-size-fits-all” diets and toward personalized protocols that account for a patient’s specific metabolic phenotype.
4. Beyond the Clinic: A Societal Shift
Obesity is as much a public health challenge as it is a clinical one. Our goal must be to bridge the gap between advanced medical science and accessible community care.
Final Thoughts
The scale tells us a number, but the Nexus tells us the story. It’s time we start reading it correctly.